CHAPTER TWO: Methodology
论文方法论 Twenty right handed healthy volunteers (10 men, mean age 26.85 years, range 21-39 years) were studied in this experiment.
2.1 Participants:
Twenty right handed healthy volunteers (10 men, mean age 26.85 years, range 21-39 years) were studied in this experiment. Participants were either staff or student of Brunel University who were recruited based on set inclusion and exclusion criteria. All subjects who were right handed and aged between 16-40 years were included for screening. Right handedness was confirmed with Edinburgh handedness inventory (Oldfield., 1971; as cited in Vines et al., 2008) ( appendix …). Each subject who met the inclusion criteria had to fill the screening form, which was intended to identify any subjects at risk.
Furthermore, subjects were assessed for the level of dexterity using self aided “dexterity questionnaire” (Appendix…) which showed that none of the participants were professional typists or musicians, as this would have affected the task performance.
The exclusion criteria was set to any individual with a history of neurological condition or neurosurgery including aneurysm clip in head or any history of heart condition including pace maker or any orthopaedic condition of upper extremity or dermatological condition of scalp and upper extremity. 论文方法论
Pregnant females were also excluded from the study. After screening the participants for study, an information sheet (appendix B) was provided to participants to inform them about the details of the study and any further doubts and questions were clarified. All participants gave their written informed consent and Research Ethics Committee of School of Health Sciences and Social Care, Brunel University approved the study.
A convenience sampling method was adopted in which subjects were invited via email and word of mouth to participate in this experiment. No incentives were given in order to minimise the subject bias. Though no sample size calculation was done, previous studies (Vines et al., 2008) have shown significant changes using less than 20 subjects. Thus, a sample of 20 healthy adults used here seemed to be sufficient for this type of preliminary pilot study.

2.2 Design: 论文方法论
It was a quantitative study, designed to investigate any measurable change in excitability of brain, IHI or motor hand function following dual hemisphere tDCS. This double blinded, randomised and sham-controlled trial compared the effect of intervention incorporating between groups design over time. Since tDCS does not produce any somato-sensory or auditory perceptions beyond an initial minute of application (Nitsche et al., 2008;
Vines et al., 2008; Gandiga et al., 2006, Hummel et al., 2005), participants could not identify if the machine was on or off. Hence, it has a strong end to validate the design of sham-controlled study. Furthermore, tDCS is a portable, non-invasive, relatively cheap, and well tolerated cortical stimulation technique with minimal side effects (Nitsche et al., 2008). Hence, tDCS was most preferable neuromodulatory technique for such lab based experiment.
All possible measures were adopted for efficient double-blinding.
The participants were blinded towards intervention by placing the tDC stimulator behind the back of subject so that the state of stimulation would not be visible to them. Each participant was identified by specific code to mask their identity. Our supervisor, who did not participate in data collection delivered tDCS while all the experimenters vacated the laboratory. He randomly assigned the participants to (1) intervention group or (2) sham group, thus, blinding researchers towards the intervention. Randomization was performed in Microsoft excel 2007 by randomly assigning numbers 1 and 2 to all participants. 论文方法论
The effect of tDCS was measured as a difference in MEP amplitude and %IHI pre and post tDCS.
Intervention group received dual hemisphere tDCS (anodal- nondominant hemisphere, cathodal-dominant hemisphere) where as sham group received tDCS only for an initial minute. Gandiga et al., (2006) reported that participants could not distinguish between real and sham stimulation with the protocol used similar to this study.
Furthermore, each participant was asked to mark how sure he/she was that tDCS was on or off on a VAS scale (visual analogue scale) of 0-10 with 0 indicating machine was 100% off and 10 as machine was 100% on (Appendix E). This was to know whether participants could identify sham stimulation, to know if sham was truly a sham condition. Each subject has to come just once for a period of two and half hours for data collection, hence no questions of subject attrition with this study design. Both TMS and tDCS has the potential to induce seizures at higher intensities, however, current strength used for this study is reported to be safe (Nitsche et al., 2008).
2.3 Apparatus:
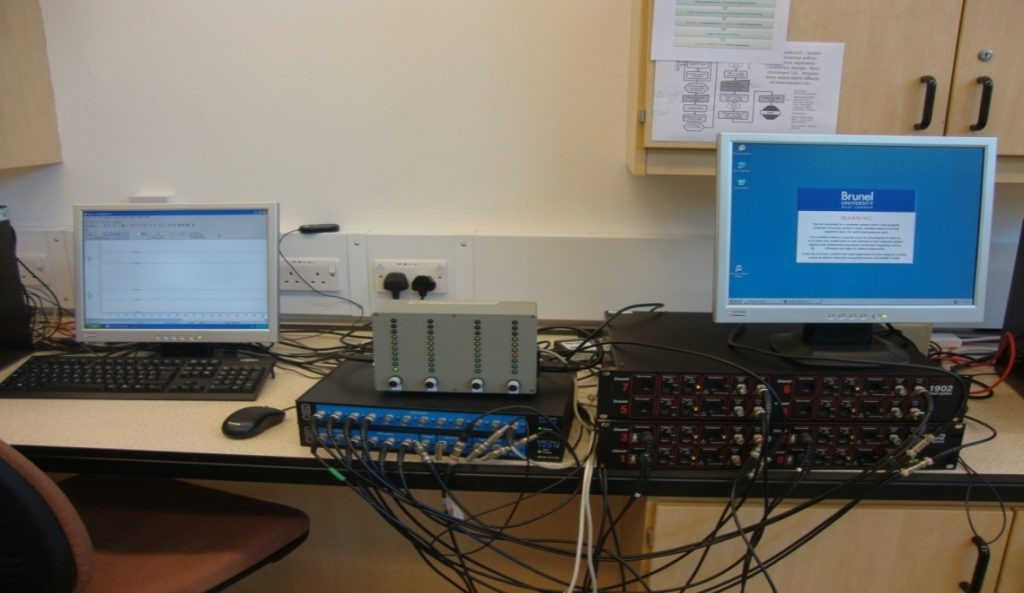
Figure 2.1: Laboratory setup
The intervention was delivered using a battery driven portable tDC stimulator (DC-stimulator: CX- 6650, model: TRCU-04A, Rolf Schneider Electronics).

Figure 2.2: tDC stimulator, CX- 6650, model: TRCU-04A, Rolf Schneider Electronics.
TMS (transcranial magnetic stimulation) was induced using Magstim 200 and Magstism-BiStim stimulator (Magstism Co.Ltd, Whitland SA34, Dyfed, UK) with a high power 90mm figure of eight coil (figure… ) (part no. 9784-00, Magstism Co. Ltd) for single pulse TMS and along with 50mm figure of eight coil for paired pulse TMS (figure… ).

Figure 2.3: Magstim-200 and Magstism-BiStim stimulator (Magstism Co.Ltd, Whitland SA34, Dyfed, UK)

Figure 2.4: 90mm figure of eight TMS coil

Figure 2.5: 50mm figure of eight TMS coil.
Transcutaneous EMG activity was recorded by disposable surface self-adhesive electrodes (ARBO neonatal ECG electrodes, Tyco Healthcare Deutschland GmbH, Neustadt/Donau, Deutschland). The acquired data was recorded and formatted in Signal 4.05 for Windows software (Cambridge Electronic Design (CED) Ltd, Milton Road, Cambridge CB4, UK). The hardware used for detection, amplification and band pass filtering was CED 1902 Quad-system Mark III (CED Ltd.) and CED Micro 1401 for digitization (CED Ltd.) (Figure 2.1).
Standard desktop computer (figure 2.1) was used for executing the finger tapping task. Task was performed on computer keyboard while visual cue for tapping appeared on monitor screen in front of the participant. Brain metric software named simple and complex motor speed measured the relevant scores including tapping speed, consistency, and number of errors.
2.4 Procedure: 论文方法论
The data collection took place in an experimental laboratory situated in Mary Seacole building of Brunel University. Subjects were made comfortable on an office chair facing standard computer desktop following screening and explaining them the data collection procedure. Anxiety level of all participants was brought down by making them aware of the sensation produced by TMS and tDCS by giving a small stimulation on their forearm.
The vertex was located using tape measure at the intersection point of the interaural line and nasion–inion connection, Cz, in 10–20 International System (Marconi et al., 2008). A distinct cross was marked on vertex which served as a reference point to locate the hotspots. Similar marking was done for both hotspots to identify their location throughout the data collection procedure. Hotspot was defined as a spot in M1, upon stimulation of which generated largest motor evoked potentials (MEP) from FDI muscle. Motor representation (hotspot) of both FDI’s in their respective primary motor cortex’s (PMC) were identified using single pulse TMS, by moving the 90mm figure of eight TMS coil systematically in 0.5 cm diameter over PMC of both hemispheres as reported by Power et al., (2006). 论文方法论
A battery-driven constant current stimulator delivered direct electric current which flowed from anode to cathode. Two surface rubber electrodes enclosed in saline dampened sponges of 25cm2 were used as anode and cathode.
Participants underwent either of the two stimulation conditions (dual hemisphere tDCS or sham tDCS) while sitting on the chair. The electrodes were placed over the motor area (hotspot) of both FDI muscles. Anode was placed on right M1 over the hotspot of left FDI and cathode on left M1 over hotspot of right FDI. Due to large surface area of the electrodes it may be possible that stimulation may have extended beyond PMC and have stimulated neighbouring area of premotor and superior parietal area as well (Vines et al., 2008).
For both stimulation conditions (ie; tDCS and sham), current was ramped up to 2mA for an initial minute and then remained on for next 14 minutes in tDCS group, but it was reduced to zero by the experimenter for sham group.The resultant current density per square centimetre of cortex accounted to be 0.08 mA/cm2. All participants tolerated the electrical stimulation well and reported to perceive it as a tingling sensation for an initial minute, which eventually felt numb. The feedback of participants on VAS scale suggests that participants of either group could not be definitive about the stimulation condition, suggesting that participant blinding towards the intervention was efficient. 论文方法论
Resting motor threshold (RMT) of both FDI’s (flexor digitorum indices) was determined by single pulse TMS which was delivered using 90mm figure of eight coil. Resting motor threshold (RMT) was defined as minimum intensity of stimulus required to evoke a 50 µV response in 5 out of 10 sweeps in a relaxed FDI (Rossini et al., 1994). To investigate IHI, two figure of eight coils were held tangentially over both hotspots with handle pointing posterior-laterally of 90mm coil and supero-laterally of 50mm coil (figure 2.6).
IHI was measured by delivering supra-threshold paired pulse TMS with 10ms delay between the test and the conditioning stimulations.
Previous studies have reported that conditioning stimulus given 6-30 seconds prior to test stimulus suppresses the EMG response evoked in hand muscle with test stimulus (Ferbert et al 1992 in Lazzaro et al 1999) .
Supra-threshold stimulus was defined as the minimum TMS intensity required to produce in at least 5 out of 10 consecutive TMS strikes an EMG response of approximately 1mV peak to peak amplitude, which came around 1.4% of RMT. This parameter was kept constant throughout the experiment. To measure IHI from the dominant to non-dominant M1, test stimulus was delivered to non-dominant M1 and conditioning to dominant M1 and vice-versa. Two sets of IHI from left to right hemisphere and vice versa were measured pre tDCS and two sets were measured post tDCS.

Figure 2.6: coil positioning while recording IHI from non-dominant (right) to dominant hemisphere (left).
A pair of disposable self adhesive surface electrodes (ARBO neonatal ECG electrodes-Tyco Healthcare Deutschland GmbH, Neustadt/Donau, Deutschland) was placed on muscle belly of FDI of both hands (figure 2.7). Ground electrode was placed over the ulnar tuberosity (bony prominence above wrist) of left hand. Electrodes were further connected to electromyography (EMG) machine to record the muscle activity generated in these muscles. Machine also provided visual feedback to subjects which assisted them to attain maximum relaxed state. The acquired EMG and MEP data was amplified by 1000 times, filtered at 1KHz–2KHz and digitalized by Cambridge electronic design (CED) 1902 in analogue with CED micro 1401 which were operated by Signal 4.05 for windows.

Figure 2.7: EMG electrodes placement while performing task B (alternate tapping).
2.5 Finger tapping tasks:
Brain Metric- simple and complex task software employed pre-designed three different finger tapping tasks of varying difficulty to assess the hand performance for accuracy, errors, speed and consistency. Prior to testing, participants had three practice trials with both hands to get familiarized to each task. A visual cue of ‘TAP’ was displayed on the computer screen in front of the participant to start tapping. Instructions for these tasks were to tap the keys as quickly and as accurately as possible. All participants were asked to position the keyboard in a manner which was most comfortable for them and maintain the same position throughout the experiment. 论文方法论
Task A (Simple tapping task) involved pressing space bar of a standard computer keyboard with index finger as fast as possible for 10 seconds. Each session had three trials which were performed alternately with each hand. Task B (complex 1) required subjects to press keys ‘S’ and ‘L’ alternately as accurately and as quickly as possible with both index fingers for 10 seconds. There were five trials of this task per session. Task C (complex 2) was the most complex task, it involved pressing four keys ‘V’’B’’N’’M’ in the same sequence with index, middle, ring and little fingers of right hand respectively and similarly pressing ‘V’’C’’X’’Z’ in same sequence using corresponding fingers of left hand. Task C was repeated five times with each hand.
All tapping tasks lasted approximately 9 minutes including short breaks of 10 seconds between each task.
2.6 Time line of study:
The complete data collection procedure is shown in figure 2.8 below. Each session lasted for 2.5 hours (150 minutes) approximately.
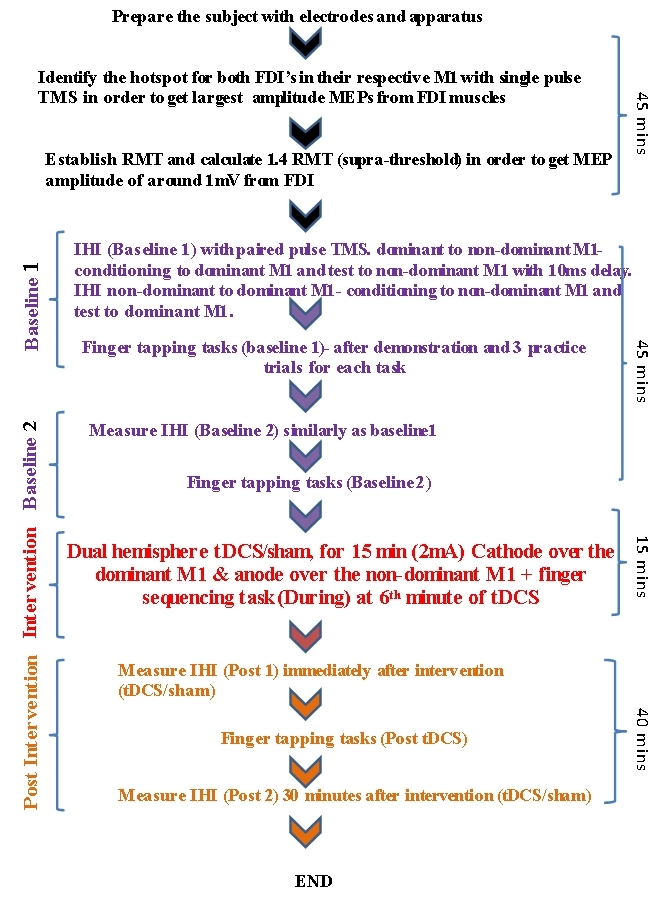
Figure 2.8: Time line plot of the data collection procedure.
2.7 Data Analysis: 论文方法论
The primary outcome measure of the study was change in %IHI pre and post tDCS and change in hand performance in finger tapping tasks, measured as number of taps and number of errors pre and post tDCS.
Brain Metric software was used to analyze the dependent variable of hand performance. The software, by itself measured and analysed total number of taps, errors, accuracy and time between each taps, which were further analysed in Microsoft excel 2007. These were compared between groups for any difference in score, pre and post tDCS over time.
The independent variable was calculated as change in MEP amplitude with test stimulus at four time frames B1, B2, P1 and P2 and compared it between groups.
Similarly, change in %IHI was observed over time including two baselines and two post tDCS and were compared between two groups for any measurable difference. Approximately 40 frames of stimulations were delivered randomly in a cycle for collecting the IHI data with 15-test only (T), 15-conditioning-test (C-T) and 10-conditioning only (C) stimuli. The frames with significant EMG activity were rejected. There were no more than 20 rejections per subject signifying that the participants were relaxed.
%IHI was determined as ratio of MEP values with mean C-T to MEP values with mean test only stimuli.
The raw data of MEP area with test stimulus and %IHI was entered in one way analysis of variance (ANOVA) to test the effect of intervention on MEP area and %IHI over time with group as a factor. One way ANOVA was run in statistical package for social science version 16.0 (SPSS 16.0, SPSS Ltd, USA). The significance value was set at 0.05. All data are reported as mean, standard deviation if not stated otherwise.
更多代写:Python代码编写 托福作弊 Online exam代考推荐 怎么写report 论文封面格式 literature review结构
合作平台:essay代写 论文代写 写手招聘 英国留学生代写